OpenLab #004: Competing at at an Ironman with Type 1 diabetes - Lucas (coachee) - Part II
Welcome back to the second part of OpenLab #004. In Part I, we covered the foundational physiology of glucose regulation in both normal physiology and Type 1 Diabetes, including the key disruptions that affect the T1D athlete at rest and at exercise onset.
Here, we build on that foundation with exercise-specific glucose kinetics, carbohydrate fuelling strategy, practical pre- and post-exercise protocols, and the real-world limits of application
Science at a Glance Continued
C) Exercise-Specific Glucose Kinetics
C.1 Moderate Aerobic Exercise (40–70% VO₂max)
In Athletes Without Diabetes
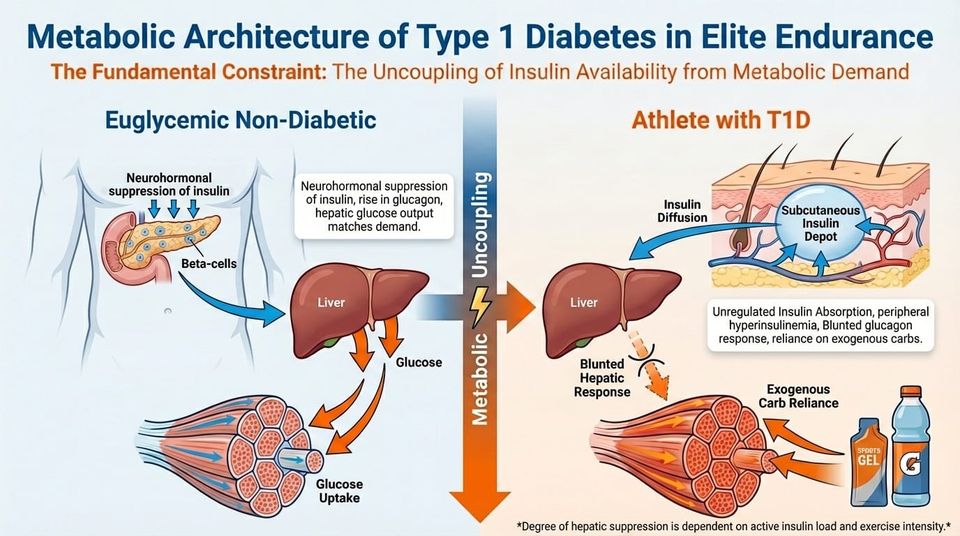
Insulin decreases rapidly, glucagon rises, and hepatic glucose output increases to match the elevated rate of muscle uptake. Blood glucose stays stable or dips only slightly.
In Athletes With T1D
Circulating insulin cannot fall quickly. Muscle contraction increases glucose uptake while hepatic output may stay suppressed by residual insulin. The result is a higher risk of hypoglycaemia. T1D athletes need to adjust basal or bolus insulin in advance, time exercise relative to dosing, eat carbohydrates strategically, and monitor glucose continuously.
C.2 High-Intensity and Anaerobic Exercise
In Athletes Without Diabetes
A large catecholamine surge drives marked hepatic glucose production, causing a temporary rise in blood glucose. Post-exercise insulin secretion then restores glycogen efficiently.
In Athletes With T1D
Catecholamines still stimulate hepatic glucose release, but insulin levels cannot adjust on the fly. Hyperglycaemia during or just after effort is common, and delayed hypoglycaemia may follow hours later as heightened insulin sensitivity drives glycogen repletion. The athlete has to manage proactively rather than relying on automatic correction.
C.3 The Intensity-Response Dichotomy
Glucose trajectory depends on intensity. Moderate steady-state aerobic exercise increases glucose uptake without a matching rise in hepatic output, pulling blood glucose down. In contrast, supramaximal efforts (HIIT, heavy resistance) trigger a catecholamine surge that stimulates hepatic glycogenolysis beyond peripheral uptake, often causing transient hyperglycaemia.
C.4 Circadian Considerations
The Dawn Phenomenon and circadian cortisol rhythms affect insulin sensitivity in meaningful ways. Morning exercise, performed when cortisol and growth hormone levels are naturally higher, often requires less carbohydrate supplementation than the same session done in the afternoon or evening, when insulin sensitivity is higher and counter-regulatory buffers are lower.
The plans you find here are built on a simple truth: Adaptation only happens when you apply the right stress, at the right time, in the right dose.
Fuelling for Performance: Carbohydrate Strategy
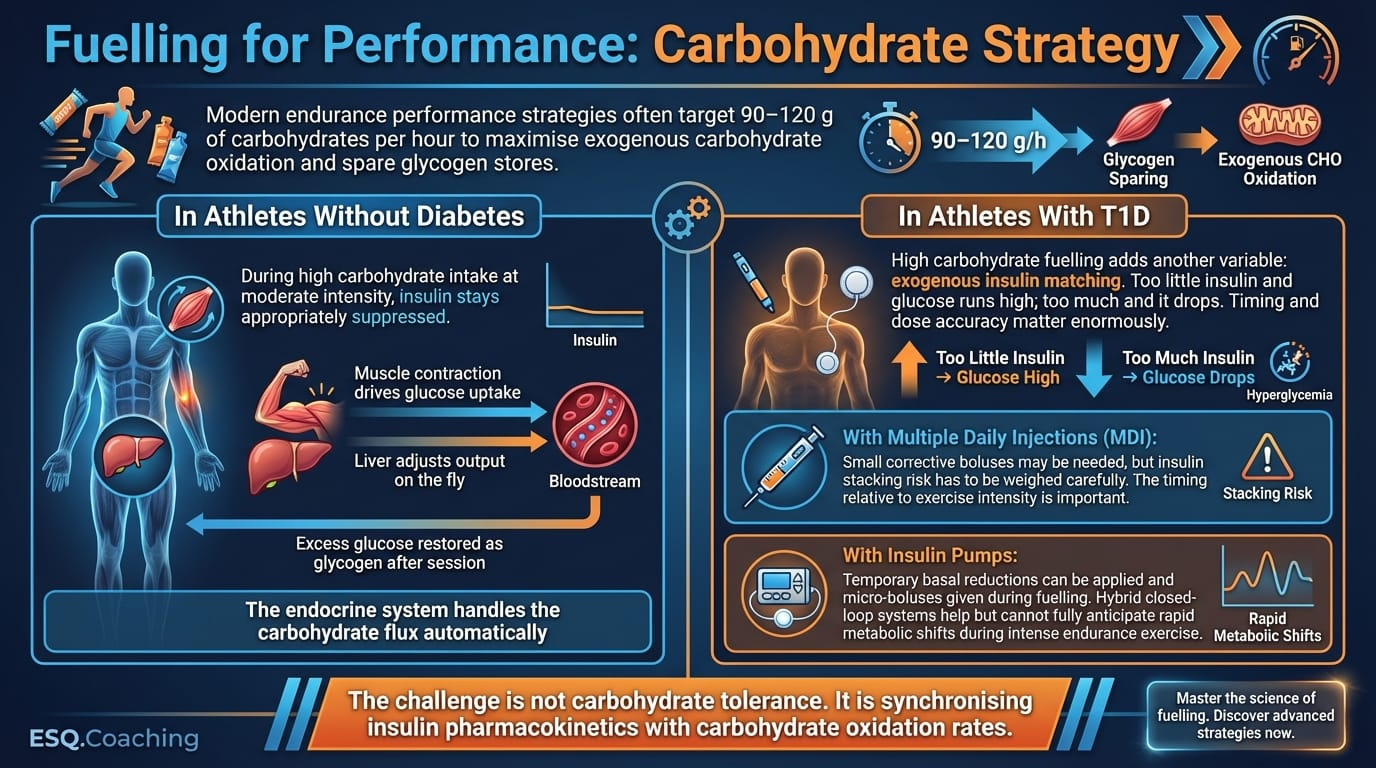
Modern endurance performance strategies often target 90–120 g of carbohydrates per hour to maximise exogenous carbohydrate oxidation and spare glycogen stores.
In Athletes Without Diabetes
During high carbohydrate intake at moderate intensity, insulin stays appropriately suppressed. Muscle contraction drives glucose uptake, the liver adjusts output on the fly, and excess glucose is restored as glycogen after the session. The endocrine system handles the carbohydrate flux automatically.
In Athletes With T1D
High carbohydrate fuelling adds another variable: exogenous insulin matching. Too little insulin and glucose runs high; too much and it drops. Timing and dose accuracy matter enormously.
• With Multiple Daily Injections (MDI): Small corrective boluses may be needed, but insulin stacking risk has to be weighed carefully. The timing relative to exercise intensity is important.
• With Insulin Pumps: Temporary basal reductions can be applied and micro-boluses given during fuelling. Hybrid closed-loop systems help but cannot fully anticipate rapid metabolic shifts during intense endurance exercise.
The challenge is not carbohydrate tolerance. It is synchronising insulin pharmacokinetics with carbohydrate oxidation rates.
Practical Protocols
Pre-Exercise Insulin Modulation
• Aerobic sessions over 90 minutes: Reduce the rapid-acting bolus by 30–75% for the meal before exercise (1–3 hours prior), depending on planned intensity.
• Pump therapy: Start a temporary basal reduction (30–80%) roughly 60–90 minutes before exercise to allow active insulin to clear.
Intra-Workout Fuelling
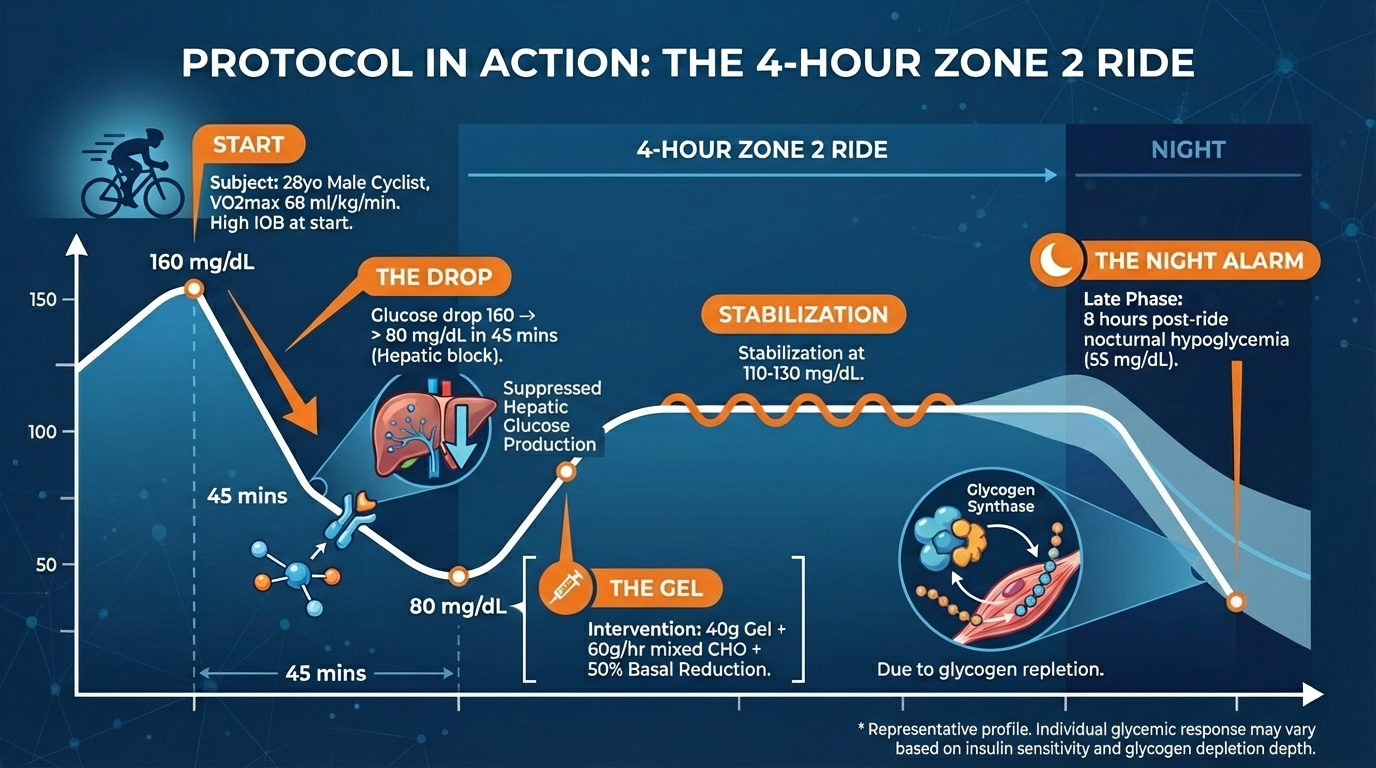
• Target intake: 30–60 g CHO/hr for moderate duration; up to 90 g CHO/hr for ultra-endurance or high-IOB scenarios.
• Timing: Start feeding immediately at onset if IOB is present. Don’t wait for hypoglycaemia.
Data-Driven Adjustment
Watch CGM trend arrows, not just absolute values. A reading of 100 mg/dL (5.5 mmol/L) with a double-down arrow calls for immediate high-glycaemic intervention, while the same value with a flat arrow may be stable.
Post-Exercise Management
• Reduce the post-workout bolus by 20–50% depending on intensity and duration.
• Watch for the biphasic drop: first, the acute decline when catecholamine support stops, and then the delayed drop from rising insulin sensitivity overnight.
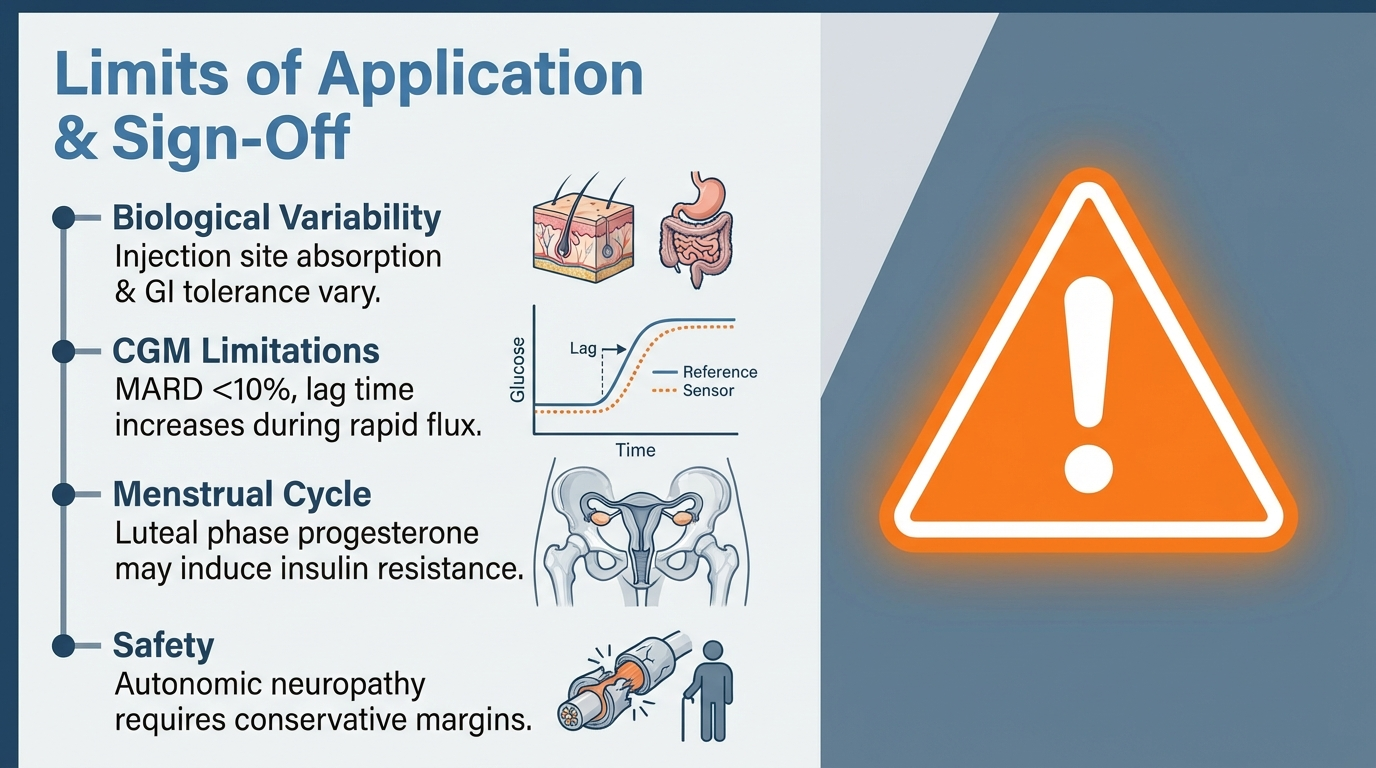
Limits of Application
This document assumes a standard physiological response to insulin and carbohydrate. In reality, there is wide inter-individual variability in insulin absorption rates (shaped by injection site and local blood flow) and gastrointestinal carbohydrate tolerance. CGM accuracy (MARD typically <10%) is generally good but can fall off during rapid glucose flux or dehydration.
Female athletes in the luteal phase of the menstrual cycle may experience progesterone-driven insulin resistance, requiring higher baseline insulin loads that complicate the reduction approaches described above.
Athletes with autonomic neuropathy may have blunted heart rate responses and reduced hypoglycaemia awareness, calling for more conservative safety margins.
Hopefully you enjoyed this #OpenLab edition and it could help you or a friend that has Type I Diabetes.
Have a great day.
Kind regards,
Lucas Fosse and Dr. Thomas Mortelmans
Legal Disclaimer
The information provided in this newsletter is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition or before starting any new fitness or nutrition regimen. The Scientist’s Notebook and ESQ Coaching are not liable for any injuries or damages that may occur from the application of the information contained herein.
References
1. Diabetes, Exercise and Competitive Sports - Gatorade Sports Science Institute
2. The competitive athlete with type 1 diabetes - PMC
3. Exercise, type 1 diabetes mellitus and blood glucose: The implications of exercise timing - PMC
4. Diabetes and Sports: Managing Your Athlete With Type 1 Diabetes - PMC
6. Exercise and Type 1 Diabetes: Must-Know Strategies for Better Control
7. Continuous Glucose Monitoring and Exercise in Type 1 Diabetes: Past, Present and Future - PMC
9. Carbohydrate Intake in the Context of Exercise in People with Type 1 Diabetes - PMC
10. Continuous Glucose Monitoring in Endurance Athletes: Interpretation and Relevance of Measurements for Improving Performance and Health - PM1. Agiostratidou, G., et al. (2017). Standardizing clinically meaningful outcome measures beyond HbA1c for type 1 diabetes. Diabetes Care, 40(12), 1622–1630.
2. American Diabetes Association. (2023). Standards of Medical Care in Diabetes, 2023. Diabetes Care, 46(Suppl. 1).
3. Bluestone, J. A., et al. (2010). Genetics, pathogenesis and clinical interventions in type 1 diabetes. Nature, 464(7293), 1293–1300.
4. Bracken, R. M., et al. (2018). Continuous glucose monitoring and exercise in type 1 diabetes: past, present and future. Biosensors, 8(3), 73.
5. Bussau, V. A., et al. (2020). The competitive athlete with type 1 diabetes. Diabetologia, 63(8), 1475–1484.
6. Cryer, P. E. (2007). Hypoglycemia in diabetes: pathophysiology, prevalence, and prevention. The American Journal of Managed Care, 13(2), 11–16.
7. DiMeglio, L. A., Evans-Molina, C., & Oram, R. A. (2018). Type 1 diabetes. The Lancet, 391(10138), 2449–2462.
8. Freckmann, G., et al. (2017). Continuous glucose profiles in healthy subjects under everyday life conditions and after different meals. Journal of Diabetes Science and Technology, 1(5), 695–703.
9. Gastaldelli, A., et al. (2000). Effect of physiological hyperinsulinemia on gluconeogenesis in non-diabetic subjects. Diabetes, 49(8), 1367–1373.
10. Horton, W. B., & Subauste, J. S. (2016). Diabetes and sports: managing your athlete with type 1 diabetes. Current Sports Medicine Reports, 15(5), 310–320.
11. Moser, O., et al. (2020). Carbohydrate intake in the context of exercise in people with type 1 diabetes. Nutrients, 12(10), 3159.
12. Munzel, T., et al. (2024). Continuous glucose monitoring in endurance athletes: interpretation and relevance of measurements for improving performance and health. Sports Medicine - Open, 10, 17.
13. Riddell, M. C., et al. (2017). Exercise management in type 1 diabetes: a consensus statement. The Lancet Diabetes & Endocrinology, 5(5), 377–390.
14. Scott, S., & Helleputte, S. (2025). Empowered: The Science of Exercise with Type 1 Diabetes. Sestante Analytics Ltd.
15. Sherwin, R. S., & Sacca, L. (1984). Effect of epinephrine on glucose metabolism in humans. American Journal of Physiology, 247(2), E157–E165.
16. Szmigiel, L., et al. (2013). Sweet 452 km: a report on the first type 1 diabetes patient to finish Double Ironman. Experimental and Clinical Endocrinology & Diabetes, 121(7), 421–424.
17. Yardley, J. E., et al. (2022). Exercise, type 1 diabetes mellitus and blood glucose: the implications of exercise timing. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 16(10), 102620.
18. Zaharieva, D. P., & Riddell, M. C. (2018). 24 days to Olympic Games: managing a competitive athlete with type 1 diabetes. Diabetes Care, 1(1), 143–147.
Found this useful?
Get articles like this and free training calculators in your inbox every week.
Recommended reads
If this was useful, these are the other research-driven newsletters I actually read.
Member discussion