Entry #017: Autonomic Regulation and HRV-Guided Training Architecture
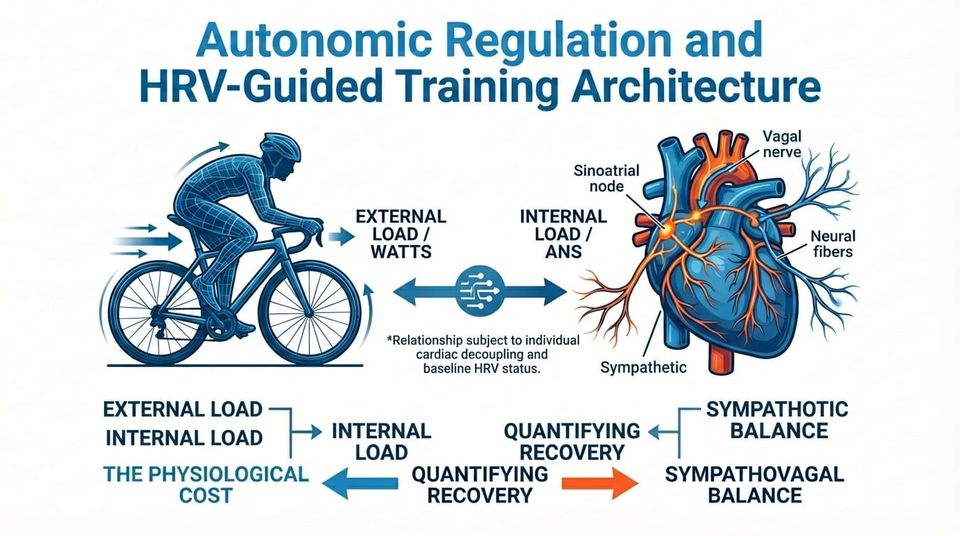
The quantification of recovery remains the most elusive variable in endurance periodization. While external load—measured in watts or pace—is easily quantified, internal load represents the physiological cost of that work and relies heavily on the autonomic nervous system's (ANS) homeostatic capacity.
Heart Rate Variability (HRV) has transitioned from clinical cardiology to high-performance sport as a primary metric for assessing cardiac autonomic modulation. However, the utility of HRV is frequently compromised by signal noise, methodological inconsistency, and the conflation of readiness with performance capacity.
This briefing examines the physiological mechanisms of HRV, critiques the validity of photoplethysmography versus electrocardiography, and outlines a decision framework for implementing HRV-guided autoregulation to optimize training adaptation.
Executive Summary – The Brief
• HRV quantifies the temporal variation in R-R intervals, serving as a non-invasive proxy for efferent vagal activity at the sinoatrial node.
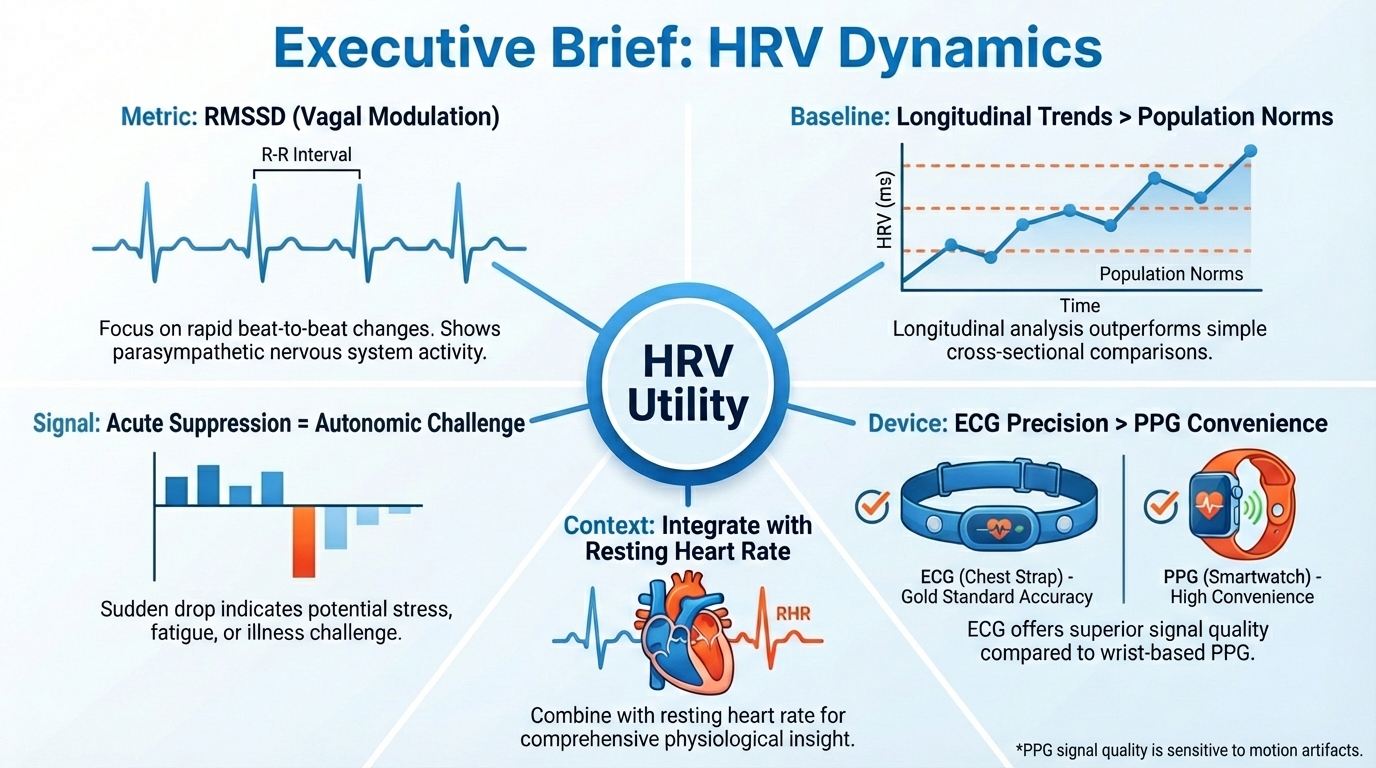
• RMSSD (Root Mean Square of Successive Differences) is the preferred time-domain metric for athletic monitoring due to its resistance to respiratory influence and strong correlation with parasympathetic tone.
• Population norms are clinically irrelevant; utility relies exclusively on longitudinal intra-individual baselines and Smallest Worthwhile Change (SWC) thresholds.
• HRV-guided training protocols consistently demonstrate superior improvements in VO2max and peak power compared to fixed periodization, often with reduced total training volume.
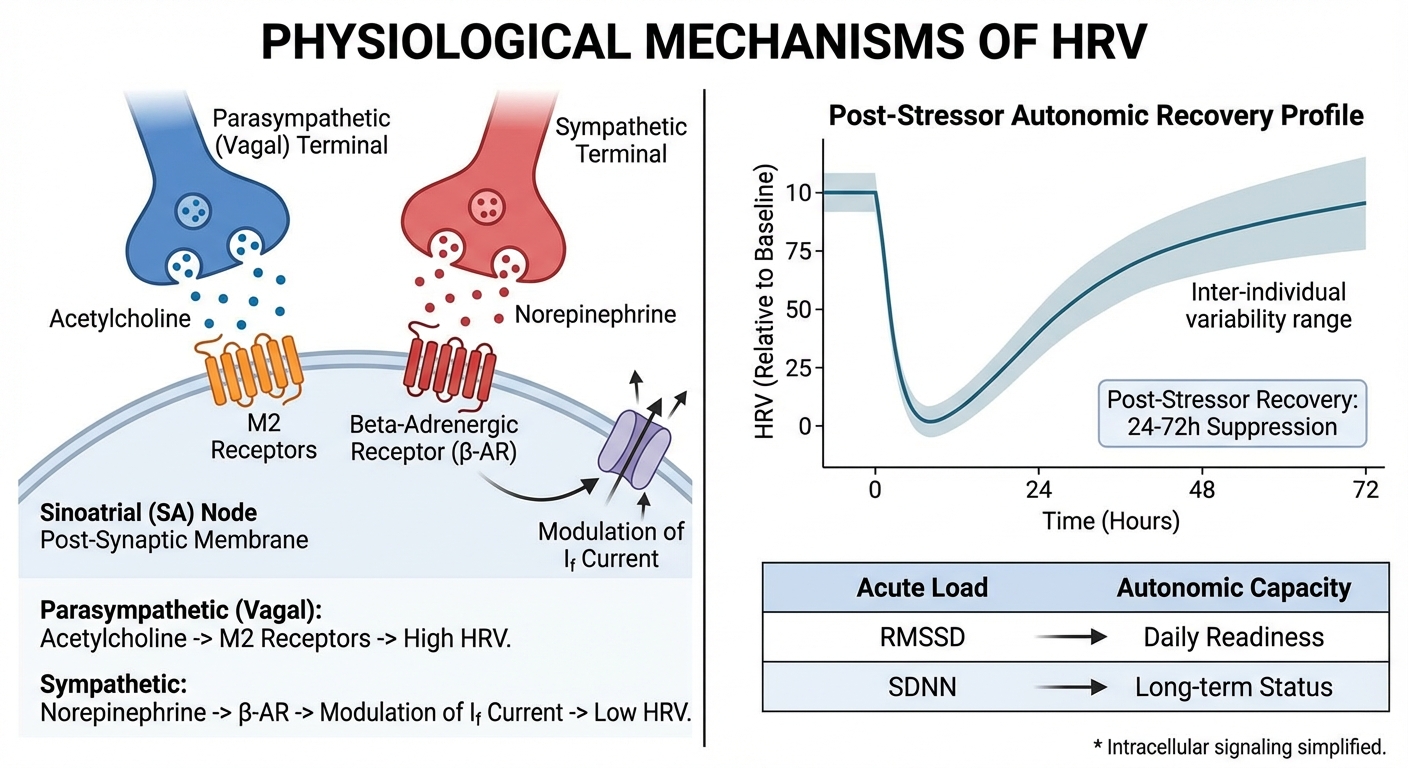
• Acute HRV suppression (24–72 hours) reflects normal homeostatic disruption following load; chronic suppression signals non-functional overreaching or systemic stress.
• Photoplethysmography (PPG) is valid for trend analysis but demonstrates lower absolute precision than electrocardiography (ECG), necessitating rigorous protocol standardization.
• Contextual integration with Resting Heart Rate (RHR) is necessary to distinguish functional recovery from parasympathetic hyperactivity.
The science at a glance
RMSSD reflects short-term heart rate variability driven primarily by vagal parasympathetic activity. The signal is dominated by high-frequency beat-to-beat variation, which makes it sensitive to acute changes in autonomic state.
In practice, RMSSD is best suited for day-to-day monitoring of recovery, fatigue, and readiness, where small shifts track sleep quality, training load, and illness. This is the most common signal, that is measured by fitness trackers (such as Garmin).
SDNN represents total heart rate variability over the recording period and integrates both sympathetic and parasympathetic influences. Because it captures overall variance rather than fast oscillations, it is less responsive to short-term stressors and more stable across time.
Its primary value lies in long-term trend analysis and population-level associations with cardiovascular and all-cause health outcomes.
The LF/HF ratio attempts to describe autonomic balance using spectral power in low- and high-frequency bands, with contributions from both autonomic branches and baroreflex activity. The metric depends heavily on recording length, breathing pattern, and analysis assumptions, which introduces large variability.
As a result, its use is largely confined to research contexts, where reliability is limited and individual interpretation is constrained.
If you want to see what I read to keep my own work sharp outside this newsletter, this is the list.
Foundational Principles
Autonomic Plasticity as a Proxy for Adaptation
HRV is not a measure of fitness, but of homeostatic flexibility. A high resting HRV indicates a system capable of rapid parasympathetic re-engagement via acetylcholine release at the muscarinic receptors.
Conversely, sympathetic dominance (driven by norepinephrine) regularizes the heart rhythm, reducing variability. This reduction signals that the system is prioritizing immediate stress response over recovery and adaptation.
The Non-Linear Recovery Curve
Recovery is not linear. Acute training stress suppresses HRV for 24 to 72 hours. This is a functional response. Maladaptation occurs when HRV fails to rebound to baseline, indicating that the allostatic load (training plus life stress) exceeds the athlete's current adaptive capacity.
Scientist’s Insight
Practitioners must be wary of 'Parasympathetic Hyperactivity.' In states of extreme functional overreaching, HRV may paradoxically rise while RHR decreases. This occurs because the sympathetic system becomes unresponsive or withdrawn, leaving the parasympathetic system unopposed. Without concurrent RHR and subjective monitoring, this signal can be misread as high readiness, leading to catastrophic training errors.
The Decision Matrix
This framework utilizes a 7-day rolling average of RMSSD compared to a 30-day baseline. It is diagnostic, not prescriptive.
(Table formatting has been reported to be broken, updating pending)
The Protocol
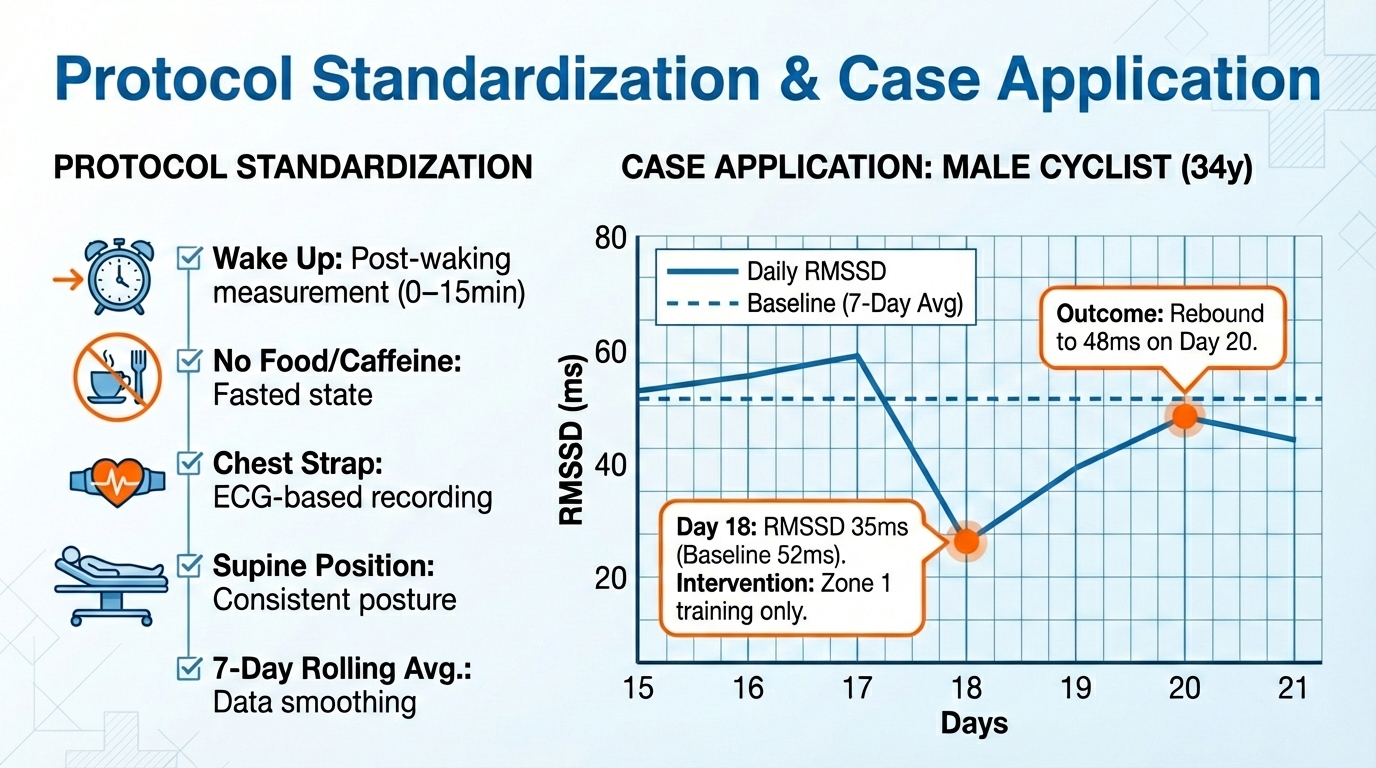
1. Standardization: Measurements must occur immediately post-waking (0–15 minutes), prior to caffeine or food intake, and in a consistent position (standing recommended for bradycardic athletes to avoid saturation effects).
2. Device Selection: Electrocardiography (chest strap, e.g., Polar H10) is the gold standard. PPG (optical) is acceptable for trends but prone to artifact from motion and vasoconstriction.
3. Baseline Establishment: Collect 4 weeks of daily data to establish the individual norm and standard deviation before altering training based on metrics.
4. Data Smoothing: Utilize a 7-day rolling average to filter daily noise. Decisions should be based on the trend relative to the Smallest Worthwhile Change (SWC), typically defined as 0.5 times the coefficient of variation.
Case Study - HRV as a guide in practice
• Subject: Male Cyclist, 34 years old.
• VO2max 62 ml/kg/min.
• Context: Week 3 of a high-volume build block.
• On Day 18, the athlete's 7-day rolling RMSSD dropped to 35ms.
• Baseline RMSSD was 52ms ± 8ms.
• RHR increased by 4 bpm.
Subjective fatigue was reported as 'mild.' Intervention: Despite the scheduled threshold intervals, the session was adjusted to Zone 1/2 aerobic maintenance. The athlete reported feeling 'blocked' during the ride. Course:
Day 19 RMSSD remained suppressed. Day 20 RMSSD returned to 48ms (within baseline). High-intensity training resumed on Day 21.
Outcome: The adjustment prevented the accumulation of non-functional fatigue, allowing the athlete to complete the block's key sessions at target power later in the week.
Note: Day 15 data was discarded due to identified ectopic beats causing a false RMSSD spike.
Power you can’t repeat is decoration.
This 8-week muscular endurance block is designed to increase how long you can hold meaningful power once fatigue is already present. Sweet spot first, control later, no wasted matches.
Choose this if you feel strong early in rides but fade when the work actually matters. View Plan here

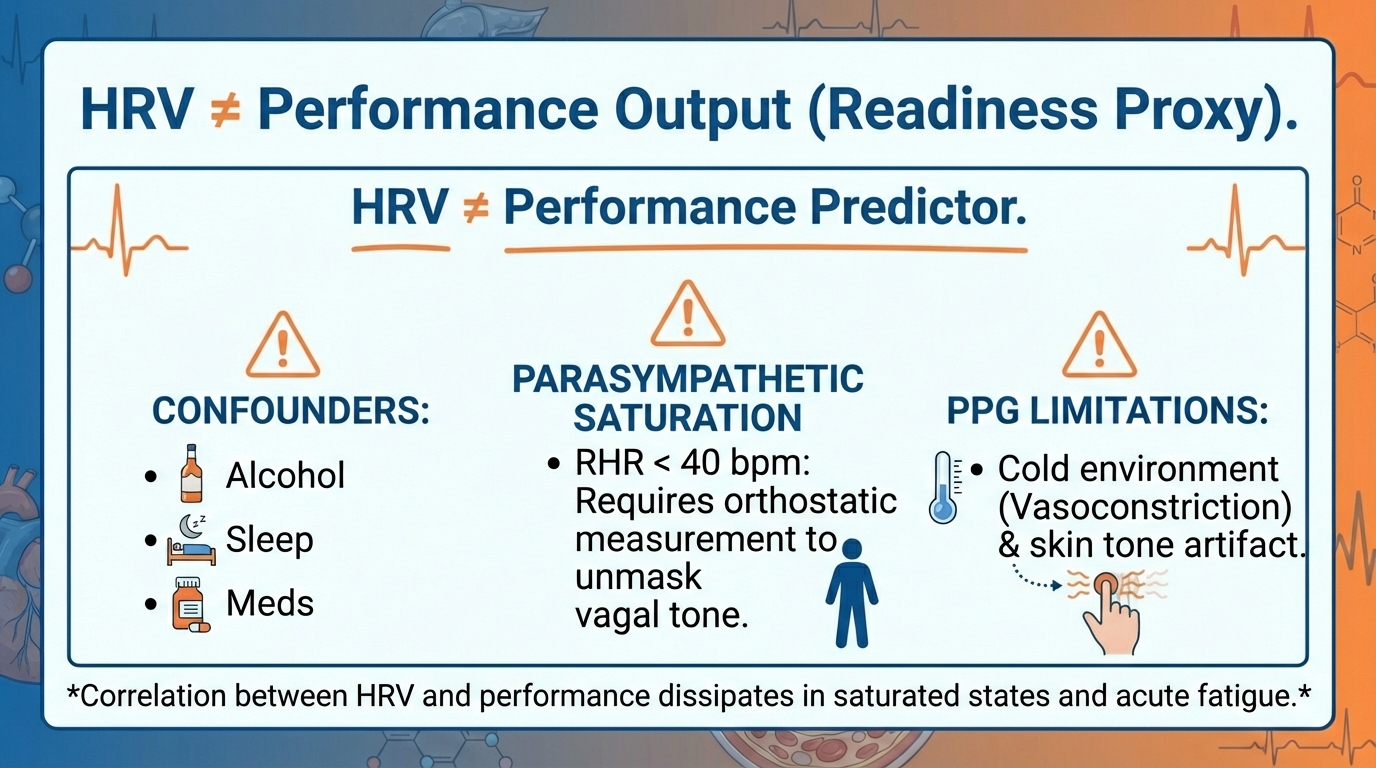
HRV is a marker of autonomic status, not a direct predictor of performance capacity; an athlete can perform well despite low HRV, though at a higher physiological cost. The metric is highly sensitive to confounders including alcohol intake, circadian phase shifts, and medication.
Furthermore, in elite endurance populations with profound bradycardia (RHR < 40 bpm), the relationship between vagal tone and RMSSD can become non-linear due to saturation effects, necessitating the use of standing measurements to induce sufficient sympathetic load for valid assessment.
Finally, PPG-based measurements may lose validity in cold environments or among populations with darker skin tones due to signal-to-noise ratio degradation.
Best regards,
Dr. Thomas Mortelmans
Disclaimer
The information provided in this newsletter is for educational purposes only and does not constitute medical advice. Exercise physiology is highly individual; what works for elite populations may not apply to everyone. Always consult with a physician before making significant changes to your training, nutrition, or supplementation protocols. The Scientist's Notebook and ESQ Coaching accept no liability for injuries or health issues arising from the application of these concepts.
References
1. Nonlinear HRV recovery and training adaptation framework | Summary: Nonlinear HRV recovery concepts in training adaptation
2. HRV-guided training guidelines and interpretation | Summary: Coach's guide to HRV monitoring for training prescription
3. HRV basics for endurance athletes | Summary: HRV basics tailored to endurance athletes
4. HRV in endurance performance: a review | Summary: Review of HRV utility in endurance training
Found this useful?
Get articles like this and free training calculators in your inbox every week.
Recommended reads
If this was useful, these are the other research-driven newsletters I actually read.
Member discussion