Entry #015: The Physiological Necessity of Time Near VO2max (T@VO2max)
In the architecture of endurance performance, a fundamental tension exists between the accumulation of low-intensity volume and the precise application of severe-intensity stimuli. While mitochondrial density and capillary proliferation respond robustly to volume, the central component of aerobic power—maximal cardiac output—requires a distinct hemodynamic stressor.
The literature indicates that simply touching the maximal oxygen uptake (VO2max) boundary is insufficient; rather, it is the accumulated time spent near VO2max (T@VO2max) that serves as the primary signal for expanding the upper limits of cardiopulmonary capacity.
For the advanced athlete, the objective is not merely to train at high intensity, but to manipulate interval kinetics to maximize time spent at >90% of VO2max without inducing autonomic maladaptation.
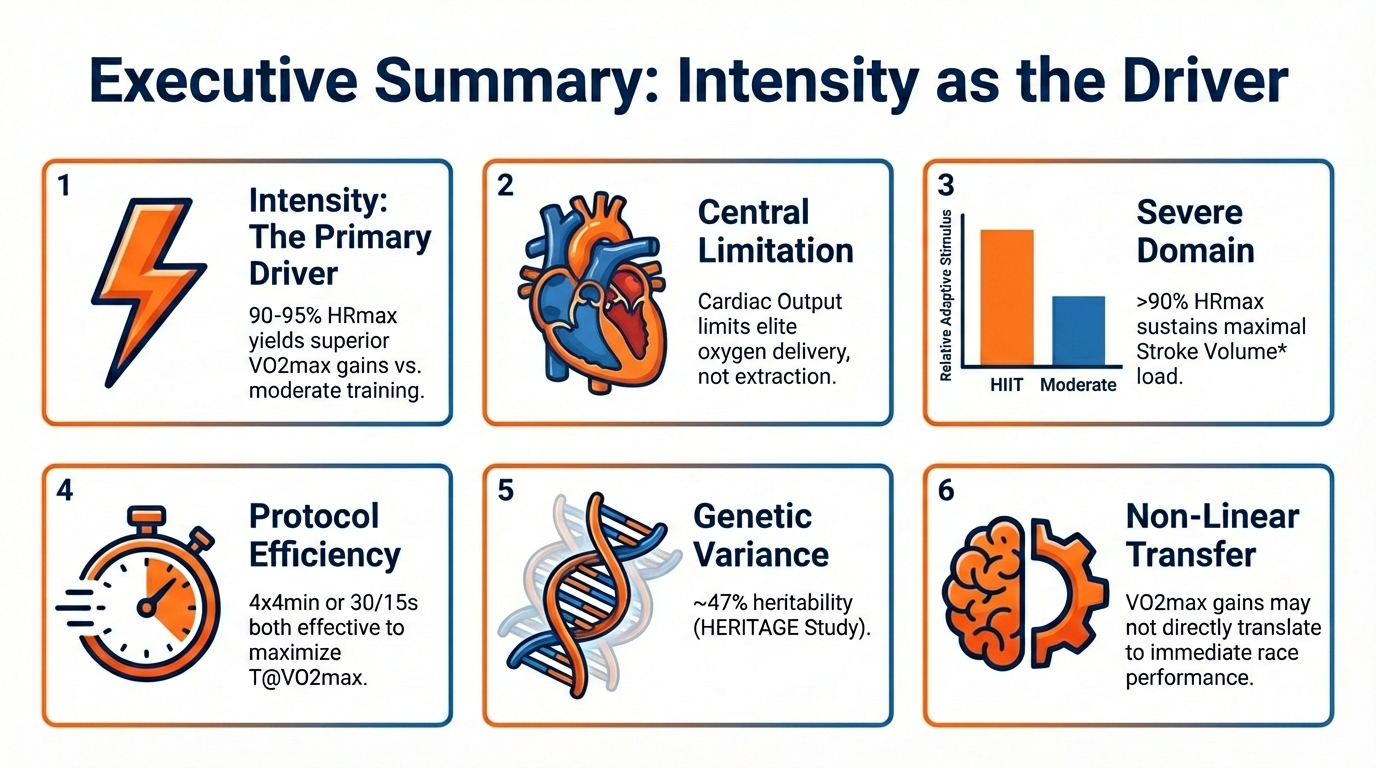
• Controlled trials demonstrate that when work is matched, high-intensity interval training (HIIT) targeting 90-95% HRmax yields superior VO2max improvements compared to moderate continuous training.
• In well-trained cohorts, VO2max is primarily limited by oxygen delivery (maximal cardiac output and hemoglobin mass), rather than peripheral extraction. High-intensity work is required to maximize venous return and challenge end-diastolic volume.
• Adaptations in maximal stroke volume occur most potently when the myocardium is subjected to maximal hemodynamic load, necessitating work rates that elicit >90% of maximal heart rate.
• Long intervals (e.g., 4x4 min) and short intervals with high work:rest ratios (e.g., 30/15s) are both effective, provided they maximize the aggregate duration the system operates at >90% VO2max.
• Improvements in VO2max do not always correlate linearly with time-trial performance due to concurrent changes in running economy and fractional utilization (lactate threshold).
• The HERITAGE Family Study indicates that approximately 47% of the variance in VO2max trainability is heritable, suggesting that apparent 'non-responders' may require significantly higher intensity stimuli to disrupt homeostasis.
The Science at a Glance
Foundational Principles
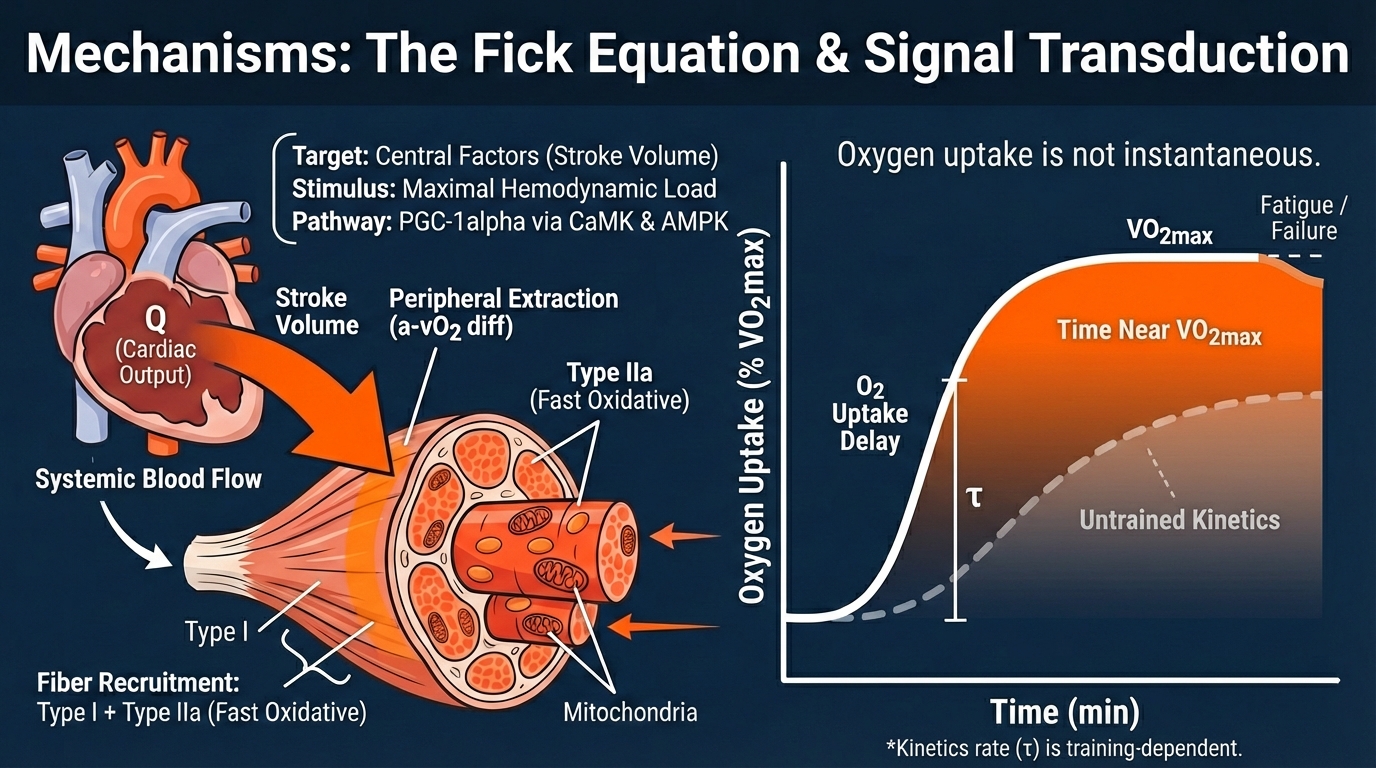
1. The Fick Equation and Central Constraints
VO2max is the product of Cardiac Output (Q) and arteriovenous oxygen difference (a-vO2 diff). In elite populations, peripheral extraction capacity often exceeds oxygen delivery. Therefore, the primary lever for increasing VO2max is enhancing maximal Cardiac Output.
This requires maximizing Stroke Volume (SV). While SV plateaus at 40-50% of VO2max in untrained individuals, it often continues to rise until near-maximal intensities in elite athletes due to enhanced diastolic filling and pericardial compliance. Thus, training must occur at intensities high enough to challenge this specific hemodynamic limit.
2. Signal Transduction via PGC-1alpha
The molecular pathway for mitochondrial biogenesis is mediated largely by Peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1alpha).
High-intensity exercise triggers distinct calcium signaling (CaMK) and AMP-activated protein kinase (AMPK) pathways that upregulate PGC-1alpha expression more potently than low-intensity volume, particularly in type II fibers which are recruited predominantly under high-force or fatigued conditions.
Scientist’s Insight: The critical metric often overlooked is not the intensity of the interval itself, but the physiological lag time (tau). Oxygen uptake kinetics are not instantaneous; there is a delay at the onset of work. Consequently, short intervals with long rest periods may fail to keep the athlete in the 'red zone' long enough to stimulate adaptation. T
The goal of protocol design is to manipulate work-to-rest ratios to minimize the drop in O2 consumption during recovery, thereby keeping the system in a state of maximal stroke volume for the longest aggregate duration.
The Decision Matrix
This framework aids in determining when to prioritize a dedicated VO2max block versus threshold or economy work.
Ceiling Limited
Raise the aerobic ceiling to create room for threshold growth.
Efficiency Limited
VO2max is adequate; focus on extending duration at speed.
Adaptation Plateau
Shift to polarized model with severe-intensity stimuli.
Autonomic Risk
1x/week micro-dose of intensity; focus on recovery.
High Fractional Utilization' implies the athlete is operating very close to their physiological ceiling. Further threshold work yields diminishing returns until the absolute ceiling (VO2max) is raised.
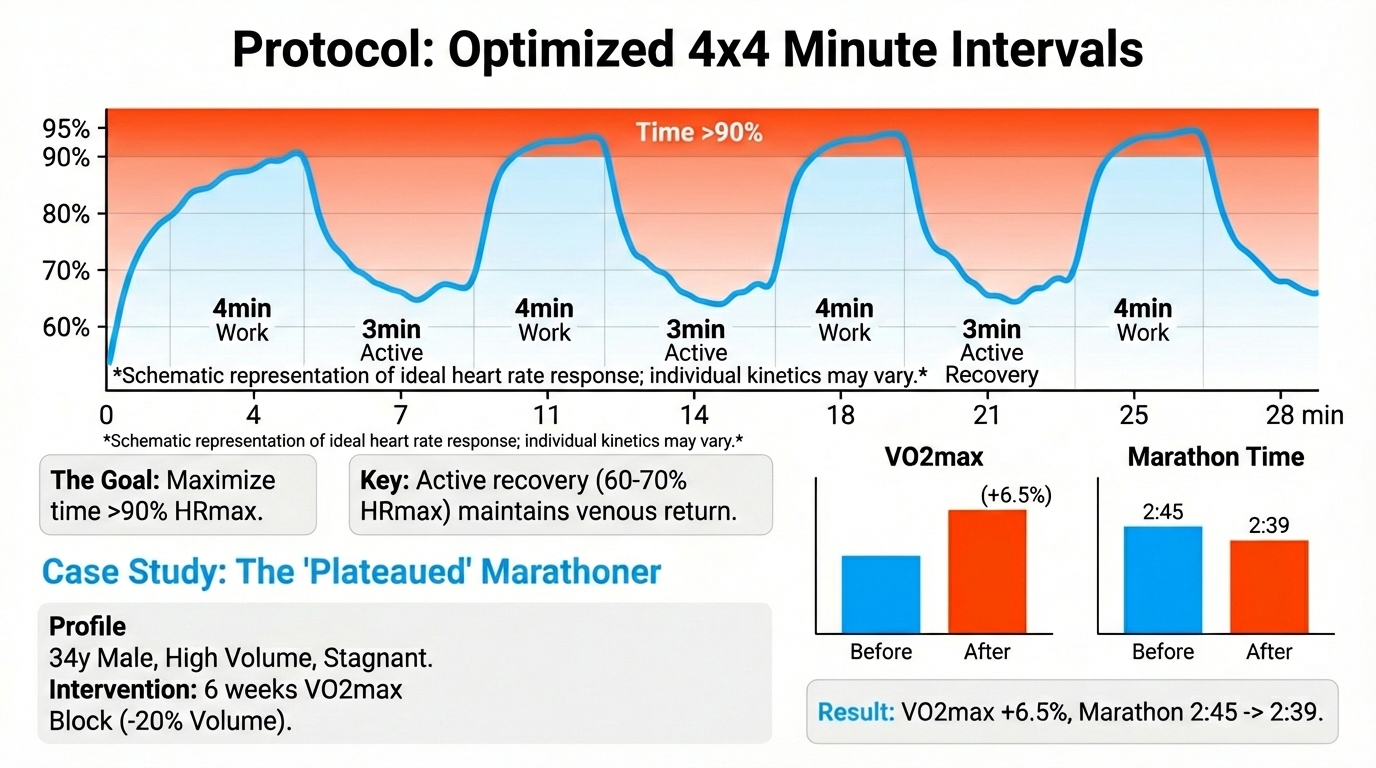
The Protocol: Optimized 4x4 Minute Intervals
Objective: Maximize time spent >90% HRmax (proxy for >90% VO2max).
1. Warm-up: 15-20 minutes progressive, including 2-3 x 30s accelerations to prime oxidative kinetics.
2. Interval 1: 4 minutes at an intensity that elicits 90-95% HRmax. Note that the first interval may require a slightly higher initial work rate to overcome O2 kinetics lag.
3. Recovery: 3 minutes active recovery at ~60-70% HRmax. (Crucial: Active recovery facilitates lactate oxidation and maintains venous return to reduce time-to-peak in the next interval).
4. Intervals 2-4: Repeat. The goal is to reach 90% HRmax faster in subsequent bouts due to incomplete recovery (cardiovascular drift).
5. Cool-down: 10-15 minutes easy.
Total Time >90% VO2max: Typically 10-12 minutes per session.
VO₂ Max Development (8 Weeks):

Your aerobic ceiling is limiting everything downstream.
This 8-week VO₂max block is for riders who already train consistently but feel capped in hard efforts above threshold. The goal is not “suffering better,” but increasing the amount of oxygen you can actually turn into power.
If long intervals feel fine but short, repeatable efforts keep breaking you, this is the block you’re missing. View plan here
Case Study: The 'Plateaued' Marathoner
Subject: Male, 34 years old, 2:45 marathoner. Training history: High volume (100km/wk), mostly Zone 2 and 'Marathon Pace' tempo.
Problem: Performance stagnant for 2 years. Lab testing revealed a high lactate threshold (88% of VO2max) but a relatively modest VO2max (62 ml/kg/min).
Intervention: A 6-week 'VO2max Block.' Volume reduced by 20%. Two sessions per week of 4x4min intervals replaced tempo runs. Low-intensity runs were slowed to ensure autonomic recovery.
Result: Post-test VO2max increased to 66 ml/kg/min (+6.5%). Lactate threshold as a percentage of VO2max dropped to 82%, but the absolute speed at threshold increased. Marathon performance improved to 2:39 in the subsequent season.
Mechanism: The intervention raised the athlete's physiological ceiling, breaking the stagnation caused by excessive submaximal volume.
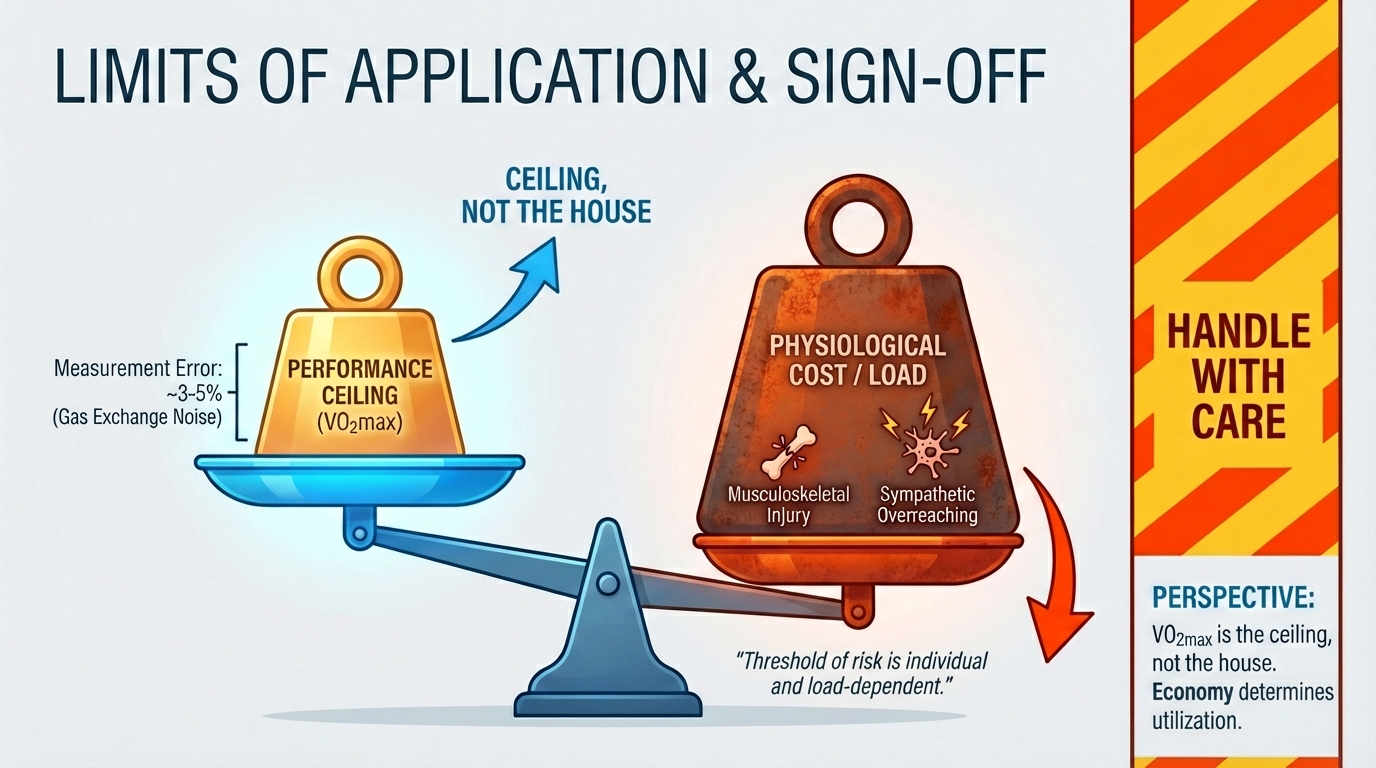
While T@VO2max is a potent stimulus, it is structurally and metabolically costly. It carries a higher risk of musculoskeletal injury and sympathetic overreaching than submaximal training. Furthermore, VO2max values derived from gas exchange analysis have a measurement error of approx. 3-5%.
Therefore, changes smaller than this magnitude may be attributed to noise. Finally, a high VO2max does not guarantee performance; velocity at VO2max (vVO2max) and running economy are often better predictors of race results in elite homogeneous cohorts. This protocol is a tool for raising the ceiling, not the entire house.
Best regards,
Dr. Thomas Mortelmans
PS: Curious to know what you liked today.Tap here for a 45-second anonymous survey. I read every single note!
Disclaimer
The information provided in this newsletter is for educational purposes only and does not constitute medical advice. Exercise physiology is highly individual; what works for elite populations may not apply to everyone. Always consult with a physician before making significant changes to your training, nutrition, or supplementation protocols. The Scientist's Notebook and ESQ Coaching accept no liability for injuries or health issues arising from the application of these concepts.
If you want to see what I read to keep my own work sharp outside this newsletter, this is the list.
References
1. VO2max and time near VO2max in endurance training | Summary: Primary VO2max determinants and training adaptations reported in early VO2max literature
2. Central vs peripheral limitations in VO2max | Summary: Central cardiac limitations highlighted in VO2max improvements
3. Effect of HIIT on VO2max in trained athletes | Summary: HIIT yields greater VO2max gains than moderate training when matched for workload
4. PGC-1alpha and mitochondrial biogenesis in response to HIIT | Summary: PGC-1alpha regulation by high-intensity exercise
5. VE-cadherin and cardiac output during high hemodynamic load | Summary: Stroke volume adaptations under maximal hemodynamic load
6. Fick equation and VO2max limiting factors | Summary: VO2max delivery vs extraction balance in elite athletes
7. O2 kinetics tau and interval design | Summary: Oxygen uptake kinetics lag and training implications
8. Lactate threshold and VO2max transfer to performance | Summary: Non-linear transfer between VO2max gains and race performance
9. HERITAGE study on VO2max trainability | Summary: 47% heritability in VO2max trainability
10. Central hemodynamics and stroke volume adaptations | Summary: Longitudinal stroke volume adaptations to training
11. Cardiovascular drift and time spent above HR thresholds | Summary: Cardiovascular drift effects on interval efficacy
12. PGC-1alpha in muscle fibers types I and IIa recruitment | Summary: Fiber recruitment differences under high-intensity work
13. VO2max determination and measurement error in gas exchange analysis | Summary: VO2max measurement error ~3-5%
14. Cardiac output as primary determinant of VO2max in athletes | Summary: VO2max limitations shift toward central factors in trained athletes
15. vVO2max and running economy predictors | Summary: Running economy and vVO2max influence performance
16. Interval protocols and time spent above 90% VO2max | Summary: 4x4 blocks and short-high intervals maximize time >90% VO2max
17. Sleep, HRV and autonomic balance in training readiness | Summary: HRV-based recovery monitoring informs training load
18. Lactate threshold and endurance performance relationship | Summary: LT2 >85-90% VO2max relation with endurance
19. Cardiac output limitations and stroke volume in elite athletes | Summary: SV adaptation maximal load
20. VO2max trainability meta-analysis | Summary: Meta-analysis of VO2max trainability across cohorts
Found this useful?
Get articles like this and free training calculators in your inbox every week.
Recommended reads
If this was useful, these are the other research-driven newsletters I actually read.
Member discussion